Breaking Mental Health Stigma
Introduction
Mental health stigma shapes silence that kills. Stigma does not only isolate people; it increases risk, obstructs care, and corrodes community trust. Mental Health Stigmas present as whispered judgments, workplace assumptions, and family taboos. Those reactions push people into private struggle. When we examine stigma closely, we find beliefs that label emotional pain as weakness, narratives that blame victims, and policies that underfund care. These beliefs remain invisible in daily conversation, yet they change outcomes in measurable ways.
Mental Health Stigma and Silent Battle
The dynamics that mental health stigma promotes within the society potentiates mental health challenge as a silent battle. People fight internal storms alone because they fear rejection, job loss, or shame. Many hide depression, anxiety, grief, or suicidal thoughts to protect relationships or reputations. Care systems then respond with gaps that are represented by long waitlists, high costs, and clinicians who lack cultural competence.
The combination of fear and poor access further turns a treatable condition into a life-or-death struggle. Families may not recognize symptoms, while friends may mistake crisis for drama. Each missed signal in turn tightens the silence.
Why Mental Health Stigma?
Reasons why there is mental health stigma around mental health challenges vary, but we can group them into cultural, structural, and narrative factors.
Mental Illness, Stigma, Silence, and Suicide
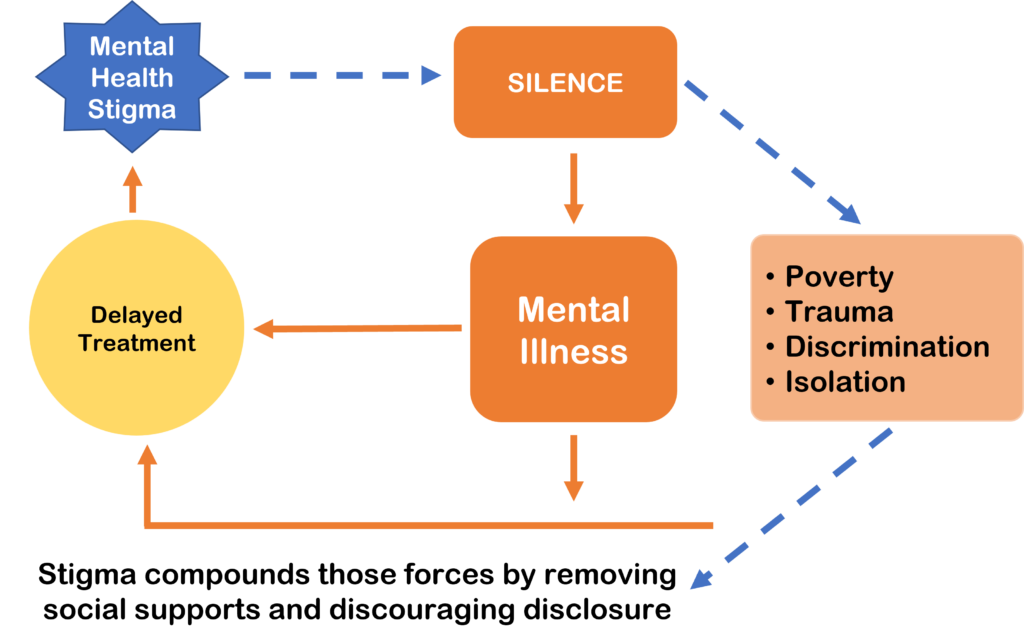
The intricate link between mental health stigma, mental illness, silence, and suicide create feedback loops. Stigma fuels silence; silence delays treatment; delayed treatment worsens symptoms; worsening symptoms raise suicide risk.
Mental illness does not operate in isolation: it interacts with poverty, trauma, discrimination, and isolation. Stigma compounds those forces by removing social supports and discouraging disclosure. When someone contemplates suicide, shame often prevents honest conversation.
Silence leaves caregivers guessing and professionals treating only surface problems. If we want to reduce suicide, we must disrupt every link in that chain.
Breaking the Mental Health Stigma Cycle
Breaking the stigma around mental health requires active strategies at individual, community, and policy levels.
Each actions, as highlighted above, move stigma from an unspoken rule to a challenged assumption. However, there are other practical steps that matter.
We must also confront uncomfortable truths: breaking stigma will not end mental illness, but it will change outcomes. When communities name pain, they free resources to treat it. When leaders speak candidly, they normalize help-seeking. When policies invest in prevention, they save lives and reduce long-term costs. This work demands persistence and compassion. It asks us to act where silence once stopped us.
In conclusion, it is worth stating that over 720,000 people die by suicide each year (For global facts and prevention guidance, see the WHO suicide fact sheet), and this is part of the fallout that mental health stigma sits at the intersection of fear and policy, culture and care. We can dismantle it, step by deliberate step. We must lead conversations, protect confidentiality, increase access, and listen without judgment. The silent battles end when people speak and communities respond. That transformation will require every one of us to trade convenience for courage and silence for steady support.

Adedeji Odusanya
Odusanya Adedeji A., is a Licensed & Certified Clinical Psychologist whose domain of expertise cuts across management of specific mental health issues such as, Depression, PTSD, Anxiety & Anxiety related disorders, Substance Use Disorder, etc